
- د. وسام 2022
- Chapter from book 2024
- د. وسام 2026جميييل 💯
- د. رحاب 2026رائع 😍
- د. خالد4 records , 6 h 😭
- د. منير
- د. أحمد عصام3½ h , ممتاز جداا
- تجميعة من د امنية
. الداتا أرشح جدا د. أحمد عصام
. شرح الكلية ممتاز والعملي هو النظري والدكاترة قالو إنهم بيشرحو النظري في السكاشن لأن المحاضرات غير كافية
أهم ال give reason 🔴🔴
McQ
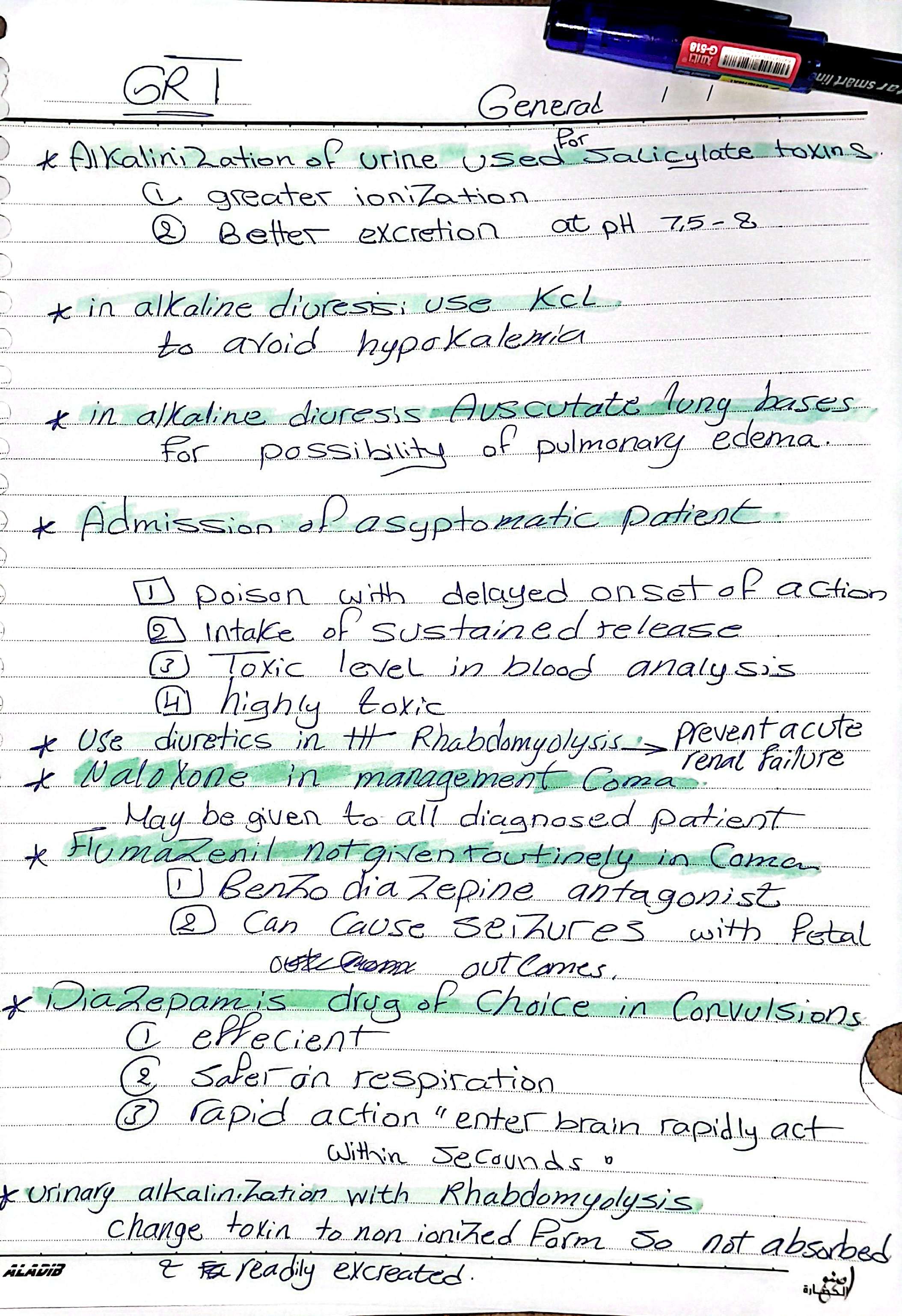
🔹Increase dose➡️more toxic effect except if vomit
🔹IV injection is the most serious route
🔹Dermal route is less serious except ( organo p+carbolic acid+tetrethlead)
🔹Causes of airway obstruction and management?
🔹come cocktail
🔹Gut emptyingcontraindications & complications
🔹Muitple dose activated charcoal (MDAC)
🔹chelator( اسمه - mechanism - route- adverse effect)
🔹antidote حالة
Naloxone➡️morfine
Paracetamol ➡️N.Acetyle cystine
Benzodiazepines➡️ Flumazenil
Atropine ➡️1) pilocarpine 2) physostigmine
🔹
حته مهمه إن ماينفعش نستخدم ال salty water as an emetic لأنه ممكن يعمل fatal hypernatremia
🔹
لو اعطي glucose قبل thiamin يسبب lesion ف الbrain
🔹
أمثلة لما يمكن عمل gastric lavage له بعد ٦ ساعات 1-anticholinergic =atropine
2- drugs which goes entero hepatic circulation
3- cocaine
4- asprine
🔹Enumerated methods of elimenation
🔺why DMSA is more prefered than BAL
🔹causes of acidosis
🔹Coma secondary to acidosis (⬇️pH).الأمثلة
🔹Coma secondary to hypoglycemia( ⬇️glucose in blood).الأمثلة
🔹Management of Coma (give reasons).
🔹toxins which cause acidosis
🔹flumazenil antidote for Benzodiazepin
🔹Why flumazenil not given with coma cocktail
🔹why benzodia safe in case of convulsion 🔹 hospital disposition.
📌 كان جاي سؤال في الايند ٢٠٢٣ ليه مش بخرج الشخص من المستشفى غير بعد 4 ساعات تقريبا رغم إنه مش ظاهر عليه أي أعراض ؟!
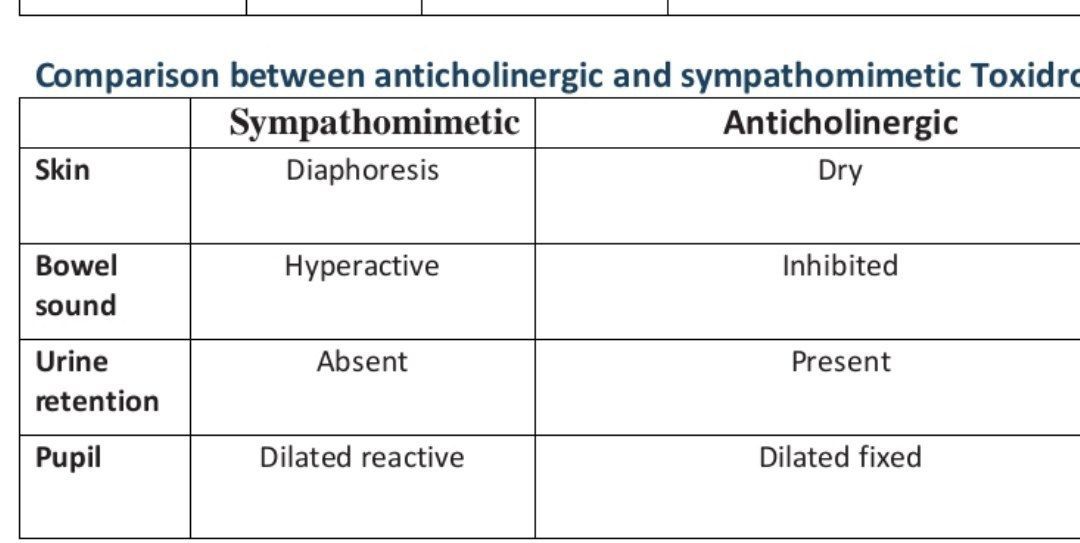
بإذن الله هؤلاء أهم give reason for toxidrome
الدكتورة ركزت عليهم قوييييي
1- Sympathomimetic drugs cause increased sweating
🔴 because they stimulate alpha-adrenergic receptors on the eccrine sweat glands.
يعني هذه الأدوية بتعمل Diaphoresis
ثاني شيء نفس الفكرة لكن تسأل عن مجموعة ثانية ألا وهي Anticholinergic تقولك ليش بتقلل العرق أو بالأصح بتعمل Dry flushed skin
بنقول:
Anticholinergic drugs cause dry flushed skin
🔴 because they block the action of acetylcholine, a neurotransmitter that is responsible for stimulating sweat glands and blood vessels in the skin.
. الداتا أرشح جدا د. أحمد عصام
. شرح الكلية ممتاز والعملي هو النظري والدكاترة قالو إنهم بيشرحو النظري في السكاشن لأن المحاضرات غير كافية
أهم ال give reason 🔴🔴
McQ
🔹Increase dose➡️more toxic effect except if vomit
🔹IV injection is the most serious route
🔹Dermal route is less serious except ( organo p+carbolic acid+tetrethlead)
🔹Causes of airway obstruction and management?
🔹come cocktail
🔹Gut emptyingcontraindications & complications
🔹Muitple dose activated charcoal (MDAC)
🔹chelator( اسمه - mechanism - route- adverse effect)
🔹antidote حالة
Naloxone➡️morfine
Paracetamol ➡️N.Acetyle cystine
Benzodiazepines➡️ Flumazenil
Atropine ➡️1) pilocarpine 2) physostigmine
🔹
حته مهمه إن ماينفعش نستخدم ال salty water as an emetic لأنه ممكن يعمل fatal hypernatremia
🔹
لو اعطي glucose قبل thiamin يسبب lesion ف الbrain
🔹
أمثلة لما يمكن عمل gastric lavage له بعد ٦ ساعات 1-anticholinergic =atropine
2- drugs which goes entero hepatic circulation
3- cocaine
4- asprine
🔹Enumerated methods of elimenation
🔺why DMSA is more prefered than BAL
🔹causes of acidosis
🔹Coma secondary to acidosis (⬇️pH).الأمثلة
🔹Coma secondary to hypoglycemia( ⬇️glucose in blood).الأمثلة
🔹Management of Coma (give reasons).
🔹toxins which cause acidosis
🔹flumazenil antidote for Benzodiazepin
🔹Why flumazenil not given with coma cocktail
🔹why benzodia safe in case of convulsion 🔹 hospital disposition.
📌 كان جاي سؤال في الايند ٢٠٢٣ ليه مش بخرج الشخص من المستشفى غير بعد 4 ساعات تقريبا رغم إنه مش ظاهر عليه أي أعراض ؟!
بإذن الله هؤلاء أهم give reason for toxidrome
الدكتورة ركزت عليهم قوييييي
1- Sympathomimetic drugs cause increased sweating
🔴 because they stimulate alpha-adrenergic receptors on the eccrine sweat glands.
يعني هذه الأدوية بتعمل Diaphoresis
ثاني شيء نفس الفكرة لكن تسأل عن مجموعة ثانية ألا وهي Anticholinergic تقولك ليش بتقلل العرق أو بالأصح بتعمل Dry flushed skin
بنقول:
Anticholinergic drugs cause dry flushed skin
🔴 because they block the action of acetylcholine, a neurotransmitter that is responsible for stimulating sweat glands and blood vessels in the skin.